
Back Pain Blues – Jim Furyk and Lizette Salas
2nd April, 2024.
Have you ever watched the video ‘Back Pain Blues’?

It shows more clearly than any doctor or movement specialist can, that golf can cause back pain! Hope you’re paying attention, golfers! The goal of this article is to inform you that YOU HAVE OPTIONS and you need not suffer indefinitely for fear of making a few (well-researched) swing changes.
Take the case of 17-times PGA Tour and 3-times Tour Champion winner Jim Furyk. He too got ‘it’. Despite a career that had limited injury (according to Mark Immelman in a recent video analysis of Furyk’s swing Since early 2022 he has been struggling with back injury, and had to withdraw from the Tour in July 2023, returning only in March 2024, just in time for the Hoag Classic at Newport Beach, California.
In the past he has said, “I’ve had some wrist surgeries and some injuries along the way, but I’ve been very, very lucky with my back throughout my career, never really had a lot of issues…I’m not really in a lot of pain, I’m just not very strong. I lost a lot of strength in kind of my right side, and I think it’s caused some bad habits in my swing.”
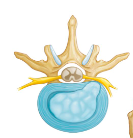
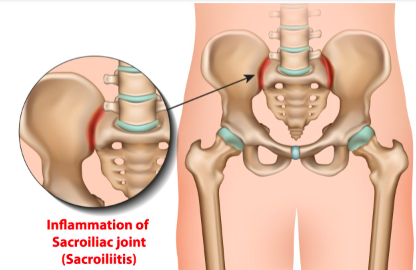
During the press conference at the start of the Hoag Classic Furyk said, “I have a couple disc issues, I had a lot of inflammation in my SI joint over the winter (pictures below). So trying to figure out – I guess put the pieces of the puzzle together trying to figure out what’s causing the pain, what’s causing my limited range of motion… I’ve worked with some doctors and had some injections done. I’ve had a lot of therapy and physical rehab, worked out a lot trying to get stronger.”
When asked whether he made any swing changes after becoming a senior to improve performance and reduce injury risk he replied, “I work with my dad a lot on my swing. I think it’s changed quite a bit in the last couple years. I watched a lot of tape on it, talked to my dad a lot about it. I think a lot of it’s out of necessity. So it’s not necessarily that we’re making changes, I think those changes kind of happen naturally. Your body’s trying to protect itself and so I’m kind of working through that and trying to get – really what I’m trying to do is gain some confidence in what I’m able to do right now. I don’t have a lot of speed in my golf swing, I’m not hitting the ball near as hard as I was say two or three years ago when I first came to this tour. I see some good flashes at times. It’s really about I think being a little more consistent right now and probably getting some reps out there where I can gain some confidence in myself.”
Herniated discs and sacroiliac joint issues are not ideally fixed by trying to get back to earlier swing patterns (the tissues of concern have deteriorated over time and now need to be treated differently going forward). Nor should they (father and son) be trying out movements without adequate knowledge of the joints, ligaments and other tissue involved. Additionally trying to ‘fix it’ by oneself takes thousands of reps to see what works and what does not, which once again is not probable during early rehabilitation. Finally, finding comfortable positions at the injured joints may lead to compensatory movements at other joints, and so any changed movements should be made around an understanding of the role of every single major joint in the body.
Many LPGA Tour players too have suffered from back injury including Nelly Korda and Lillia Vu. Lizette Salas of Azusa, California, is a 12 year ‘veteran’ of the LPGA, has won on the Tour twice, and represented the USA in five Solheim Cups. She is a former Trojan from the University of Southern California and, at the LPGA’s recent Media Day, announced that she will return to golf after many months of rehab to participate in the J M Eagle LA Championship presented by Plastpro event at Wilshire Country Club in April 2024. It is, after all, in her hometown and the event has raised much excitement amongst LPGA players because the sponsors, Shirley and Walter Wang, have raised the purse to a whopping $3.75 million.
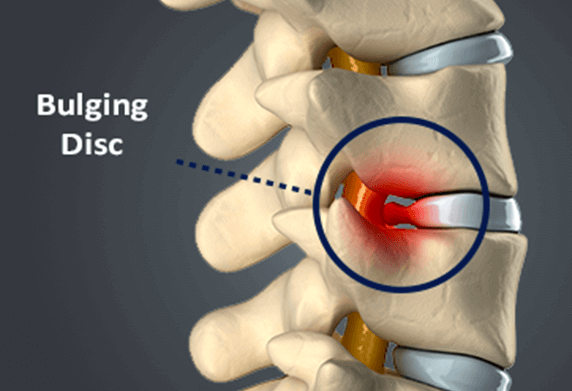
Talking very frankly about her injury, Salas said, “I’ve suffered from back pain on and off probably since my rookie year, but nothing that severe. It was pretty scary. A pain that gradually got worse. Met with some doctors and tried to put a ‘band-aid’ on it so I could keep playing and then it got pretty bad to which I couldn’t tie my own shoe – it was pretty painful and not the best time.” When prompted she revealed, “I had two bulging discs (L4-L5 and L5-S1, see pictures below) and some muscle weakness in my upper mid-back that we also had to address. So the first 2-3 months it was how did this happen and how can we make a plan and stick to it. They tested me in many different ways mentally and physically. A lot of painful physical therapy, a lot of needles, a lot of doctors’ appointments, so I got a taste of our health care system,” laughs, “But I’m glad that part is over and I can come back and play golf.”

Are the discs back in place now? “They’re stable”
Did you make any swing changes to help with the pain? “Not necessarily swing changes, I think we just identified what my tendencies were that maybe can cause more pain down the road. Some early extension that could irritate some discs in the long run. We came up with a good practice routine – to be more efficient. I can’t really grind the way I used to. My coach and trainer know me really well so I’m on a strict ball count which means I can only hit 70 balls a day. I’ve grown up to that!”
“We just know that golf is very hard on our bodies. I don’t think we’re biologically built to be in those positions. It’s a very grueling sport, especially if you’re doing it at high speeds.”
So true. Basically the golf swing should be built around what the human body can do, rather than the body being expected to perform around some hypothetically good swing.
As Salas kindly shared the names of her medical team (two orthopedic surgeons, two physical therapists and a massage therapist), it was easy enough to get in touch with one of them. Dr. Alex Weber, orthopedic surgeon at the USC Keck School of Medicine agreed to answer a few questions.
Do you regularly work with golfers or was Lizette Salas an exception? “Our patient population tends to be some golfers – not exclusively golfers – but we see our fair share of professional golfers and also many recreational golfers.
How do athletes know to go to you specifically? How does that workout if you don’t mind sharing ? “Some of the professional athletes come to us via their agents or through connections in their world and others come to us through other means.” He has known Lizette for some time at he is on the Trojans’ medical team and she has played for the team.
If you have a pro golfer of Lizette Salas’ level, with herniated discs, what are your most favorite rehabilitation and return to play (RTP) protocols?
“We try really hard to avoid the operating room and even try to avoid injections and focus really hard on the rehab and return to play by spending a lot of time working on core strength and stability as well as glute and hamstring and quad activation and strengthening and that plus some lower extremity lumbar flexibility for most athletes gets them back to full return to play without any additional interventions.
“The way our system typically works is we have them see physical therapists and a rehab specialists, and I’m certainly not against them using the alternative forms of medicine too. So if they’d like to see a chiropractor, massage therapist, acupuncturist, I think all those things are great and we typically check in periodically to make sure that they’re progressing and meeting the milestones and working towards a full recovery.
Are you personally very conservative in your return to play recommendations because Lizette said she’s worked up to hitting 70 balls a day! That’s practically nothing! “You can call it conservative but I think once the core strength and flexibility is there, we do let athletes progress as they feel comfortable but certainly we always try to be cautious and not have setbacks. I think the best rehabs and recoveries are those that are linear and we just don’t want to have setbacks. So as long as the athletes are pain free and progressing that’s what we really care about.”
So all these athletes are working out 2-3 hours with their personal trainers. How come they still get injured and then what is the difference in the exercise modalities that you prescribe? “It’s a good question. I think sometimes with athletes there is overuse so you said they work out 2-3 hours a day, but maybe they also hit balls 2-3 hours a day. So they workout in the gym 2-3 hours a day, they work on flexibility an hour and sometimes maybe sleep gets a little bit disturbed, or they’re not eating perfectly and so all of these variables when taken together sometimes can lead towards injury. When they’re having back issues we pull back on the amount they’re in the gym and those 2-3 hours turn into rehab hours.”
Do you or anyone in your in your team such as the physical therapist or chiropractor recommend any swing changes? “I stay as far away from swing changes as possible – I think that sometimes those conversations come up with physical therapists or rehab specialists but certainly that’s way outside of my area of expertise so I leave that stuff alone.”
You’re not a golfer at all? “I’m actually a decent golfer.”
This seems to be a great irony – in every sport the coach is someone with zero relevant educational background. They’ll have some degree in English or some degree in philosophy and they are teaching movement with no background in human movement and you guys are the experts – the expert of experts – and yet you don’t tell them these are the movements that are causing the problems – that’s so surprising! “It’s a good question and I know exactly what you’re saying, I appreciate what you’re saying very much. You know how golfers are about their swings and swing is a very sensitive topic. I think if there are things which are markedly off in the athletes’ movement pattern certainly we help correct those and that’s coming through the physical therapist and the rehab specialist. Those are the people who are really highly trained in movement and movement performance and they’re the ones who can help correct movement patterns, more so than the orthopedic surgeon.”
Basically, then, golfers, the facts are as follows:
1. Golf injuries are common and perhaps getting more common (there has been no epidemiological study in golf for over 15 years) with recent popular changes. Changes that have been made in an attempt to achieve better so-called ‘use of the ground’!
2. Overuse combined with known injury-causing mechanisms is the biggest culprit for golfers. Traditionally, it has been believed that less skilled athletes have ‘poor mechanics’ and more skilled ones simply have ‘overuse’. That is NOT the case. All mechanics that cause injury or inconsistent performance, regardless of skill level, should be deemed ‘inappropriate mechanics’. If golfers can get rid of the injury-causing mechanisms they could, perhaps, extend the life of delicate tissue, despite overuse.
3. Golfers appear to either be scared of swing changes or do not know/believe changes can help their situation
4. There is an urgent need to have a golf instructor-scientist-manager (GISM) on every injured elite golfer’s team. Almost like an air traffic controller who can bring together all the relevant aspects for the injured golfer. The goal being to return the athlete to golf without excessive delay, and with the ability to perform well and in as pain-free a manner as possible.
The role of the GISM expert in the team:
1. Conduct a detailed, independent analysis of swing positions and motions (full swing and short game), from both an anatomical and a mechanical perspective
2. Discuss the injuries with surgeon, physical therapists/chiropractors, rehab specialists to get an understanding of the injured tissues and laterality (left or right side of injury, very important in golf) and the planned rehabilitation steps
3. Discuss relevant weaknesses/strengths of the athlete with nutritionist, fitness trainer, sports psychologist to understand required steps going forward
4. Make suggestions to the athlete and the team, including recommended swing changes.
Any swing changes decided upon MUST be scientifically researched so as to no longer ‘play around’ with the athlete’s health and performance.
The swing changes I recommend are based on research of over 30 years. My LPGA Master Thesis https://jacc-ojs-twu.tdl.org/jacc/article/view/201901 involved looking through 869 research papers, and provides information on epidemiology and etiology of golf swing injury. Tissue-wise details of etiology of low back pain may be seen on pages 24-27.
With the recommended swing changes:
• Movement is reduced, not increased, and the swing, overall, is much simpler. Thus performance faults are fewer and easy to identify.
• The slightly different set-up triggers the new swing so a golfer is not stuck between two different movements and able to randomly produce either one!
• The set-up positions and backswing motions lock out the golfer’s ability to make dangerous movements such as over-the-top, early extension, excessive clubface rotation through impact.
A basic, from-internet-only view of Furyk’s swing , suggests that (pictures below) he has too much downswing side-bend and rotation, which, combined, have been referred to as the ‘crunch factor’ and were known, as far back as 1998, to be injurious to golfers. One of the reasons for his excessive side bend is that he reroutes his arms and club from the top of the backswing, which requires a repositioning of the torso. Additionally, he slides his pelvis and knees towards target during impact, so that his dynamic balance is off and he must add additional side-bend to his trail side to stay in balance. He also has excessive downswing torso rotation, perhaps from learning golf at a time when rotation was considered to be vital for speed development.


The main solution for him would be to stabilize the upper and lower body during the backswing.
Lizette’s swings show that she has a short, steep backswing that reroutes (involving sidebend) halfway through the downswing, requiring fast torso movement to pull off.


The solution for her would be to lengthen her backswing (not easy to do from a traditional set-up and backswing), so that the arms drop down before torso motion is initiated. This allows stretched muscles to contract easily rather than using force to abruptly change torso direction.
There is always a way, golfers. A few simple swing changes make for a far better solution than months or years lost from long-term physiotherapy or even surgery!